")
(Part 24 of Dr. Pagtakhan’s column on Medisina at Politika.)
Introductory Quotes
“If the virus not only replicates but also manages to spread, human to human, among a few dozen other individuals, that’s an outbreak. If it sweeps through a community or a country, that’ an epidemic. If it encircles the world, it’s a pandemic.” - David Quammen, Author of “Spillover: Animal Infections and the Next Human Pandemic”
---
It has been a year of anguish and longing for optimism since COVID-19 began its global circulation. It has caused monumental damage to living and livelihoods and exacted enormous human toll on health and life. Worldwide, the magnitude of disease has surpassed the 100 million ark and the gravity of death has exceeded 2 million. Canada’s shares of the burden stand at 772,441 sickened and 19,739 deceased. These have been the grim hallmarks of this pandemic until the recent availability in Canada, USA, the U.K. and the European Union of the Pfizer/BioNTech and Moderna and vaccines. Optimism has never been greater. - Dr. Rey D. Pagtakhan: January 28, 2021
Let me look back on the year past as COVID-19 unfolded to share what we have learned from our one-year experience covering the pandemic: our understanding of the disease and of the many issues that have surrounded it.
A year ago, today, the Canadian Filipino Net (CanFilNet) published ‘Novel Coronavirus Infection: Information and Guidance’ to alert its readership to this then new respiratory disease, which emerged in Wuhan City, China, on December 8, 2019 as a cluster of 11 patients with pneumonia of unknown origin. When the cluster became an outbreak of 59 patients, China notified the United Nations World Health Organization (W.H.O.) about this new disease on December 31st.
A week later on January 8, 2020, Chinese scientists identified the viral pathogen and posted online its genetic sequence.This posting helped start the early development of mRNA vaccines against COVID-19 and, thereby, saved years that would have otherwise been needed. On the 12th, W.H.O. confirmed that a novel coronavirus was the cause of undiagnosed pneumonia.On January 13ththe first case outside China was confirmed in Thailand on a resident who had just returned from Wuhan.
W.H.O. declares highest public health alert
On January 30 – barely a day before press time for our inaugural issue of February 1-15 on this new viral respiratory disease – W.H.O. announced it as a public health emergency of international concern.
Both CanFilNet and Pilipino Express have covered the evolution of this globe-trotting agent of acute respiratory disease and death since our February 16, 2020 issue when we noted the initial grim statistics for China: 42,670 patients sickened, 1,018 deceased, and over 60 million residents quarantined in their homes and apartments.
Travel as the early mode of spread
The first cases seen in Canada during the first and last quarters of 2020 had come, like the first case in Thailand, via international travel: from Wuhan, Qatar, Egypt, Philippines, and USA. One of the other two first cases came from another province and one from a cruise ship. Subsequent transmissions occurred between community members.
Canada's National Microbiology Lab: Early in the evolution of this pandemic, this Lab in Winnipeg performed the diagnostic testing for COVID virus on samples from suspected cases sent by provinces and territories, either as the sole test or as a check of an in-province test result. The first confirmed case in Canada was diagnosed by the lab on January 27, 2020. Since then, provinces and territories have established their own testing capacity but have occasionally sent samples to the national lab for a second test as a check.
We have developed a much better understanding of the virus and the disease - which now have their official names, SARSCoV-2 and COVID-19, respectively. We have a better appreciation of its impact in all its aspects – social, financial and economic - on individual patients, their family, community, and country.
The severity of infection varies from mild, moderate, severe to critical based on their signs and symptoms and their need for oxygen and mechanical ventilators to help in breathing. Nearly 80 per cent (80%) of the infection are mild, including the nearly half of whom (40%) without sign and symptom. The moderately-severe to critical group – nearly 20% of the total infected – have posed a high disease burden, have overwhelmed hospitals and intensive care units and health care workers, and exposed the insufficiency of protective personnel equipment supply.
It takes on average five days after exposure and almost always before the end of the 14th day to develop the signs and symptoms. This is the incubation period and it relates to the symptomatology caused by the virus, not to its transmissibility. In fact, infected people are already able to spread the virus before symptoms appear. Moreover, even those who never go on to develop the disease – they are called asymptomatic carriers – are contagious.
On March 12, W.H.O. officially declared the world’s 6th pandemic - the first time that a member-virus of the coronavirus family has caused a global epidemic.Within 100 days from its start, its geographic spread has reached all regions of the U.N. health agency, six continents, and 114 countries, affecting over 100 thousand patients and causing over 4 thousand deaths. At this juncture, Canada experienced a hundred-fifty-fold increase in new patients during a preceding two-week period. So much so that Canada’s whole-of-government response to the disease established “more than $1 billion COVID-19 Response Fund…to limit the spread of the virus in Canada and prepare for its possible broader impacts.”
All provinces have declared either a public health or state of emergency or both for a 14-day duration at the onset of Spring, enabling them to put in place public health tools of social distancing: enforceable ban on mass gathering, closure of recreational facilities, withdrawal of non-essential public services, limits to travel, home quarantine, stay-home directive, and directives to maintain 2-meter distance. Breach of these measures incurred fine and/or jail term.
While the federal government kept its option on the national Emergencies Act open, it focused on 1) imposing 2-week self isolation on all upon arrival from international travels; 2) providing vital economic and funding package for citizens, businesses and the medical research community; and 3) reinforcing the need to stay home and maintain physical distancing. The aim was to prevent overwhelming burden on our health care system.
We have since learned that acquisition of SARSCoV-2 virus can result in different clinical outcomes among individuals in the same risk group: 1) respiratory failure and death; 2) severe pneumonia and recovery on oxygen therapy, with or without ventilator; 3) mild pneumonia and spontaneous recovery at home; and 4)asymptomatic carrier who may not even be aware and only detected when tested as a contact.
We still do not know why the differences in response following exposure to the same virus.
For example, it is still impossible to predict who will end up as an asymptomatic carrier spreading the virus or who will succumb from the infection. This uncertainty and unpredictability should help guide us as we receive directives from public health authorities.
We have been introduced and reminded about the need for hand-washing and provided with hand-rubbing diagrams to ensure proper techniques, including duration of the entire procedures, to ensure effectiveness.
We have recognized that the pandemic has been unsettling times particularly for children and youth when their usual geographic landscapes outside the home are closed to them: daycare, nursery, and kindergarten classes; grade and high schools; colleges and universities; playgrounds, parks and beaches; restaurants and bars; movie theatres and concert halls; and places of religious worship. Their respective anxieties and apprehension for themselves and for their siblings, parents, grandparents, cousins and their friends would be awakened. Teenagers in particular are vulnerable.
Lockdown, self-isolation, quarantine,stay-at-home,shelter-in-place,six-foot physical distancing,and no handshake. These have become a common part of our daily lexicon. Parks, playgrounds and beaches closed; vacations and trips cancelled; schools, colleges and universities interrupted; prom and graduation ceremonies, birthday celebrations and weddings postponed; no sports, movie theatres, nor concerts; restaurants and bars closed. These most certainly add stress to daily living.No visitors to senior’s home; healthcare workers getting infected and dying, ER and ICU overwhelmed; test kits not enough; conflicting and confusing messages from government officials and leaders; place of worships closed. These touch the soul and humanity of anyone.
By late Spring, we heard the First Ministers’ Joint Statement on Re-starting the Canadian Economy.We were advised that if we lifted measures too quickly, we could lose the progress we've made. Hence, we set the criteria and measures needed to restart the economy, namely, that:
- COVID-19 transmission is controlled;
- Sufficient public health capacity is in place to test, trace, and isolate all cases;
- Expanded health care capacity exists for all patients, COVID-19 and non-COVID-19;
- Supports are in place for vulnerable groups/communities and key populations;
- Workplace preventative measures are in place; and
- Risk of importation of infection is lessened.
Knowing more about virulence of the virus and unusual symptoms and signs
Before summer ended, we came to know even more about the virulence of this virus. That it could inflict damage, directly or indirectly, almost anywhere in the human body from head to toes with very serious consequences: persistent pain or pressure in the chest; bluish lips or face, and stabbing headache; repeated shaking with chills, muscle pain and state of exhaustion; loss of taste or smell and seizures; anorexia, nausea, and vomiting; disorientation, inability to arouse or stay awake, delirium and falls; red or purple rash resembling frostbite (“COVID toes”); exceedingly low blood oxygen levels without the accompanying breathlessness (silent hypoxia) ; and signs and symptoms of severe stroke (numbness, weakness of extremities, sudden difficulty with words and speech).
Understanding these unusual symptoms provides new insights to front line workers and carry implications for patient care. The difficulty in breathing that we normally attribute to lung damage might actually be defects in the control of breathing by the nervous system. The presence of neurological symptoms – loss of taste or smell – could alert the attending doctor into who might go sooner into acute respiratory failure and, thereby, and help in triaging of patients.
New and repurposed prescription drugs
There are now two medications: remdesivir for adult and pediatric patients hospitalized with severe pneumonia and requiring oxygen therapy. The second drug is dexamethasone. - already an existing drug in use for other clinical conditions. While it has now been recommended for hospitalized COVID-19 patients on mechanical ventilators or supplemental oxygen, note has been made that the drug may be harmful if given for less severe COVID-19 infection. Evidently, the arrival of the two medications (the new remdesivir and the old repurposed dexamethasone) for a particular phase of hospitalized COVID-19 patients has prevented a number of deaths that would have otherwise occurred.
At on set of summer, we featured a photo-image of former US President Jimmy Carter – a Nobel Peace Prize recipient – and first lady Rosalynn Carter while explaining the rational use of face mask or cloth face covering to help prevent to any degree achievable the further spread of COVID-19:
- The COVID-19 virus easily spreads between infected people even before symptoms appear or without ever developing any;
- The virus can spread through talking or even just breathing in addition to sneeze/cough-induced droplets;
- Heavy breathing and singing can propel aerosolized viral particles farther than two meters (6 feet) and thereby increase the risk of transmission;
- Infectious viral particles could linger in the air for hours and later inhaled;
- Incubation period is long – up to 14 days – and thereby give a wide window of opportunity for people, even before they know they are infected, to infect others; and
- Carriers may be most contagious in the 48 hours before they show symptoms, making transmission even more blind.
Thus, people who look well can have and spread the virus. When they shout, cheer and sing loudly, they produce a lot of droplets and aerosolization and enhance their infectivity. The fact that a person with COVID-19 virus, on average, can spread it to two or three other people makes it twice as contagious as the common flu. Anyone in this type of situation – and that can include anyone of us – is a potential spreader.
While masks are primarily intended to reduce the emission of virus-laden droplets (“source control”), which is especially relevant for asymptomatic or presymptomatic infected wearers who feel well and may be unaware of their infectiousness to others, they also help reduce inhalation of these droplets by the wearer (“filtration for personal protection”).
Children in the eye of the pandemic storm
We have come to appreciate that children are very much in the eye of the pandemic storm.
When hospitalized, as many as a third (32%) of the patients required oxygen therapy, half of whom also needed a ventilator. That they could develop serious sequelae, such as severe inflammatory syndrome.
Schooling and college
As Fall appeared, we focused on the impact of the pandemic on schooling for children and back to college for young adults. While there was a nearly universal chorus to bring children safely back to school even in the midst of COVID-19, there was at the same time some very strong dissonant voices against mandatory in-person instruction without flexibility. I have never observed such intensity of deeply held opposing viewpoints about school re-opening from my reading of the mainstream media; position statements of pediatric associations; and guidelines from W.H.O., Public Health Agency of Canada and USA Centers for Prevention and Disease Control; as well as from medical and scientific reports on the burden of the pandemic on children.
Why some college students break COVID-19 rules
We were reminded that collegiate rites of passage to adulthood encourage youth to take risks to find new connections. Restrictions to behavior could only lead to rebellion. That’s why fraternity and sorority bid days at the start of the semester are accompanied by mass gatherings and parties, rules against them in the age of COVID-19 notwithstanding.
We were reminded, however, that risky behaviors may be a function of their normal physiological and emotional development, not a conscious breach of prescribed public health rules. This much we have learned from developmental psychologists, whose advice includes the following approach:
- Colleges and universities need to share with students the responsibility of keeping those on campus safe; shifting blame onto students could stir up rebellion;
- Stir students to appreciation of mutual benefit and sacrifice and motivate everyone's buy-in to take care of each other; and
- Handle them with empathy and acknowledge the sacrifices they have already made to help control humanity’s crisis; summon up the best in them.
COVID-19 and influenza duo
As we prepared for the Fall and Winter seasons and realized the arrival of the seasonal flu in the midst of the COVID-19 pandemic would make for a fearful duo, we brought to the attention of the community the dual threats – the co-occurrence of the two contagious respiratory illnesses in the same patient. We offered the needed advice: Get the flu vaccine at the first opportunity. It is our best protection against the fearful duo.
It was around this time that we experienced the surge of cases and wondered whether we were seeing the second wave of the pandemic. We remembered: The historic influenza pandemic of 1918-1919, also known as the Spanish flu, showed three waves. Its highly fatal second wave accounted for most of the American deaths attributed to it. This is the reference being made when we speak of COVID’s second wave and its dreaded severity. But the Spanish flu’s greater severity was due to the mutation of the virus to a more virulent strain. Presently, the occurrence of variant strains has very much been on the news channels.
The wide circle of tragedy
We learned about the “wide circle of tragedy with every COVID-19 death,” that is, no death is ever just ‘a number.’ Bereaved children get pushed into or near poverty and risked foster care placement after deaths of parents. That applying a “bereavement multiplier of 9 for every death,” as developed by researchers at the Penn State University, we would appreciate the gravity of the current toll of deaths in Canada and in the world. That long-term impacts and disabilities do exist: long-term damage to patients’ lungs, heart, immune system, and brain. That as much as a third of the patients who recovered had difficulty breathing and unusual fatigue months after their diagnosis and as much as close to 89% of recovered patients had “abnormal findings on cardiovascular imaging.
Unprecedented Times in Vaccine Development
Near the end of summer, 14 vaccine candidates anticipated clinical testing. In particular, Moderna and Pfizer appear working at an unprecedented speed. Their products would eventually receive emergency use approvals in Canada, USA and Europe last December. Said Gary Kobinger – the director of the Infectious Disease Research Center at the Université Laval in Quebec City: “It’s actually important to test a lot of vaccines. If we could have five vaccines that are safe and work and are potent, that would be much better. It reduces the chances for manufacturing bottlenecks. With five vaccines, maybe we could manufacture enough for everybody on the planet.”
Joyful winter with vaccines: That two safe and effective vaccines, Pfizer/BioNTech and Moderna, – each with average efficacy of 95% - would become available for use come December was more than a welcome major tool to help control the preceding alarming surges of cases immediately prior to vaccine availability. Wrote Drs. ER Rubin and DL Longo in their editorial on the Pfizer/BioNTech‘s COVID-19 vaccine in the New England Journal of Medicine (December 12, 2020 issue): “What appears to be a dramatic success for vaccination holds the promise of saving uncounted lives and giving us a pathway out of what has been a global disaster.”Summed up the editorial: “The level of safety the vaccine has demonstrated thus far is remarkable. With this number of participants and this follow-up period, safety does not arouse specific concern.”
How exciting it was, indeed, to know that Canadians, together with Americans, Britons and citizens of the European Union (EU) and 15 other countries, have finally begun their mass immunization against COVID-19 to curb the unrelenting increase of new cases and deaths from this pandemic. This sets the stage for ending the acute pandemic realistic before the end of the new year.
Vaccination update
How many of the supplied doses have been injected: As of January 27th, 868,454 of the 1,122,450 vaccine doses supplied (77.37%) to provinces and territories have been injected, ranging from 30.5% in the Yukon to 94.4% in Quebec and even to 104.1% in Saskatchewan. The province found 104.1% efficiency from the allocated supply by drawing extra doses from the vials. The total administered doses reflect 2.29% vaccination rate for the total Canadian population, ranging from 0.91% in Nova Scotia to 21.01% in the Northwest Territories. Data from all individual provinces and territories can be found in the Public Health Agency of Canada website.
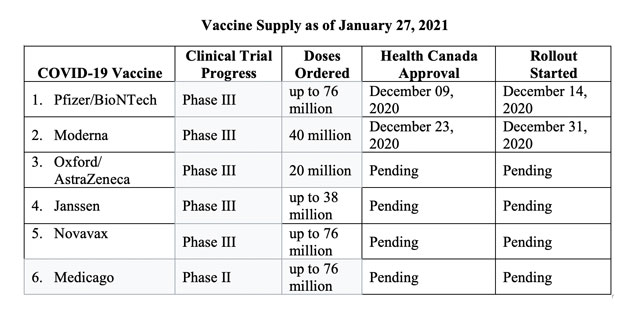
Vaccine supply: Vaccines are projected to come from six suppliers as shown in the Table below, including status of their rollout:
Delay in delivery from Pfizer/BioNTech: No sooner have we asked ourselves to temper our optimism and news of delays in vaccine delivery has been announced. Next delivery from Pfizer would not come as originally scheduled “due to the continuing manufacturing disruptions at its facility in Belgium,” reported Paula Newton (CNN News, January 20, 2021). Prime Minister Justin Trudeau is quoted reassuring Canadians that “the overall goal, to have every Canadian vaccinated by September, would be on track”. However, the overall decrease over the next month could be as much as half as originally planned. Said Maj. Gen. Dany Fortin, the commander in charge of the vaccine rollout, "There will be a considerable impact across all provinces."
Understanding why it is hard to make vaccines and boost supplies?
Lauran Neergaard (AP News, Jan 28 2021) has summed up the answers to this question: Many detailed steps and ingredients of supplies go into the manufacture of vaccines. Add to that the millions of doses in demand and one sees the enormous challenge faced by manufacturers. All countries are asking for their fair share of supply. In response, pharmaceutical firms are retooling their factories and have to produced their supplies at volumes needed. No wonder the recent news about delays in shipment of the earlier promised doses. The process of producing a vial of vaccine requires meticulous care – any little refinement needed causes delay. Different vaccines require different technologies, raw materials, equipment and expertise. Creating mRNA is an involved chemical process and not as easy to translate from a small to super-large volumes. Working with biologic ingredients faces variability. And all the steps in the production must follow strict quality control procedures to ensure the quality of each batch. To help alleviate the delay, Pfizer and Moderna are expanding capacity.
Knowing these particulars require of us patience than unnecessary belligerence.
The current situation on cases and deaths
Drop in cases: Except in Nunavut where there is an increase, there has been a drop of new cases per 100,000 population (per 100K) across Canada from 1.00% drop in B.C. (that is, nearly a plateau) to 100% (that is, no case seen) in Prince Edward Island; the pan-Canadian average drop is 18.00%. Total cases per day per 100K remain high in the following five provinces in descending order: Quebec (2,985), Alberta (2,753), Manitoba (2,095), Saskatchewan, (1,922) Ontario (1,756) and British Columbia (1,267).
Number of cases: Globally, the total number of cases has reached 101,687,508 with the following 10 countries sharing the greater burden: U.S. – 25,793,302; followed by India and Brazil in the 9-to-10-million range; Russia, United Kingdom and France – each in the 3-million range; and Spain, Italy, Turkey and Germany – each in the 2-million range. Canada’s share of the burden comes to 772,441 – the 22nd place among countries; Philippines at 521,413 makes it to the 32nd position.
Number of deaths: Globally, 2,195,871 citizens have lost their lives to the disease, with U.S. nearing half a million (433,719). Canada’s and Philippines’ share stand at 19,739 and 10,600, respectively.

Editor's note: Dr. Rey D. Pagtakhan, P.C., O.M., LL.D., Sc.D., M.D. M.Sc. is a retired lung specialist, professor of child health, author of articles and chapters in medical journals and textbooks, and a former health critic, Parliamentary Secretary to the Prime Minister, and cabinet minister, including Secretary of State for Science, Research and Development. He graduated from the University of the Philippines, did postgraduate training and studies at the Children’s Hospitals of Washington University in St. Louis and University of Manitoba in Winnipeg, and spent a sabbatical year as Visiting Professor at the University of Arizona Medical Center. In June 2003, he spoke on “The Global Threat of Infectious Diseases” at the G-8 Science Ministers/Advisors Carnegie Group Meeting in Berlin.